Introduction
Cardiovascular disease is the leading global cause of death, accounting for 17.3 million deaths per year, a number that is expected to grow to more than 23.6 million by 2030(1).
- Cardiovascular diseases claim more lives than all forms of cancer combined.
- About 85.6 million Americans are living with some form of cardiovascular disease or the after-effects of stroke(1).
- Direct and indirect costs of cardiovascular diseases and stroke total more than $320.1 billion. That includes health expenditures and lost productivity.
- About 610,000 people die of heart disease in the United States every year–that’s 1 in every 4 deaths(2).
- Coronary heart disease (CHD) is the most common type of heart disease, killing over 370,000 people annually(2).
- Every year about 735,000 Americans suffer from a heart attack. Of these, 525,000 are a first heart attack and 210,000 happen in people who have already had a heart attack(2).
Who should be tested?

Ideally to be tested are:
1. Asymptomatic patients (i.e. showing no symptoms) at intermediate risk (10-year risk of atherosclerotic cardiovascular disease, 5 to 20 percent).
2. Selected patients with a family history of premature coronary artery disease and a 10-year risk of less than 5 percent(3)(4).
Relevance:
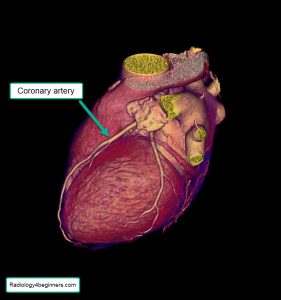
Coronary artery calcium (CAC) is a highly specific feature of coronary atherosclerosis. On the basis of single-center and multicenter clinical and population-based studies with short-term and long-term outcomes data (up to 15-year follow-up), CAC scoring has emerged as a widely available, consistent, and reproducible means of assessing risk for major cardiovascular outcomes, especially useful in asymptomatic people for planning primary prevention interventions such as statins and aspirin(5).
CAC testing in asymptomatic populations is cost-effective across a broad range of baseline risk(5).
Furthermore, subclinical atherosclerosis assessed by using CAC is associated with an increased future likelihood of regional wall motion abnormalities, as a marker of previous and possible subclinical coronary artery disease(6).
CT-based abdominal aortic calcification is a strong predictor of future cardiovascular events, outperforming the Framingham risk score. This finding suggests a potential opportunistic role in abdominal nonenhanced CT scans performed for other clinical indications(7).
We use the Agatston score to do this assessment(8)(9).
For demonstration purposes, I have below examples of three patients with various risks. We will start with the patient with the lowest risk of having a significant coronary artery disease, and then work our way up to the patient with a very high risk of developing coronary artery disease. These three patients were investigated on the same day in our institution.
Patient 3 (Agatston score of 0)
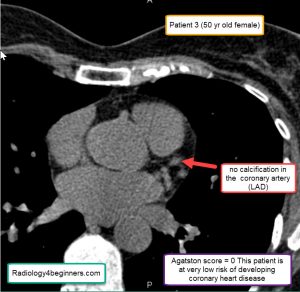
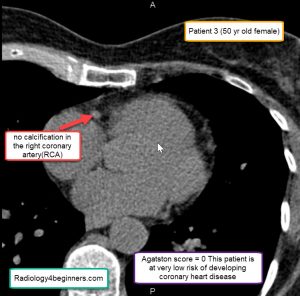
This patient was really concerned about having a significant coronary heart disease. He has had recent chest pains and has a family history myocardial infarction (heart attack). After the scan, we were able to reduce his anxiety and send him home smiling.
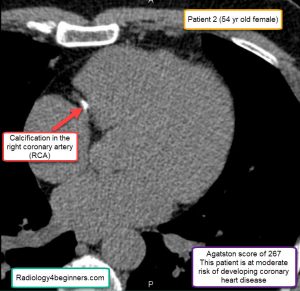
Patient 2 (Agatston score of 267)
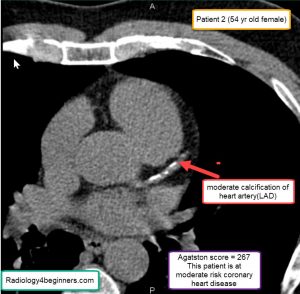
This patient is at moderate risk of developing coronary heart disease
This patient is at moderate risk of developing coronary heart disease
Patient 2 has a family history of coronary artery disease. Her father died of myocardial infarction(heart attack) at the age of 55. She is at a moderate risk of developing coronary artery disease. She needs aggressive risk modification i.e. smoking cessation, adequate management of her diabetes, weight reduction, etc. She would also need to do additional tests like a cardiac stress test.
Patient 1 (Agatston score of 1400)
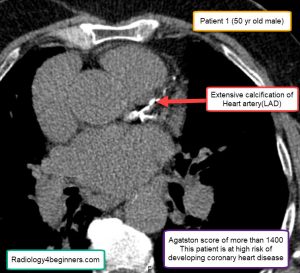
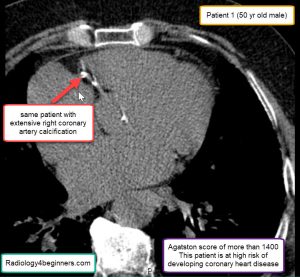
Patient 1 is a chain smoker, drinks a lot of alcohol and also has diabetes with high blood sugar levels. He admitted to not having been taking good care of himself recently because of some life-changing events.
Selected reading
- DM, EJ B, AS G, DK A, MJ B, MC, et al. Heart Disease and Stroke Statistics – At-a-Glance. Am Heart Assoc. 2015;
- Centers for Disease Control and Prevention. Heart Disease Facts & Statistics | cdc.gov. U.S. Department of Health & Human Services. 2018.
- Hecht H, Blaha MJ, Berman DS, Nasir K, Budoff M, Leipsic J, et al. Clinical indications for coronary artery calcium scoring in asymptomatic patients: Expert consensus statement from the Society of Cardiovascular Computed Tomography. J Cardiovasc Comput Tomogr. 2017;
- Hecht HS, Cronin P, Blaha MJ, Budoff MJ, Kazerooni EA, Narula J, et al. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: A report of the Society of Cardiovascular Computed Tomography and Society of Thoracic Radiology. J Thorac Imaging [Internet]. 2017 Sep [cited 2019 Nov 1];32(5):W54–66. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28832417
- Greenland P, Blaha MJ, Budoff MJ, Erbel R, Watson KE. Coronary Calcium Score and Cardiovascular Risk. Journal of the American College of Cardiology. 2018.
- Colletti PM, Dustin LD, Wong ND, Shriki JE, Detrano RC. Association of Subclinical Atherosclerosis with Left Ventricular Systolic and Diastolic Dysfunction at MR Imaging in an Elderly Cohort. Radiology. 2010;257(1).
- O’Connor SD, Graffy PM, Zea R, Pickhardt PJ. Does nonenhanced CT-based quantification of abdominal aortic calcification outperform the Framingham risk score in predicting cardiovascular events in asymptomatic adults? Radiology. 2019;290(1):108–15.
- Van Der Bijl N, Joemai RMS, Geleijns J, Bax JJ, Schuijf JD, De Roos A, et al. Assessment of Agatston coronary artery calcium score using contrast-enhanced CT coronary angiography. Am J Roentgenol. 2010 Dec;195(6):1299–305.
- Criqui MH, Denenberg JO, Ix JH, McClelland RL, Wassel CL, Rifkin DE, et al. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA – J Am Med Assoc. 2014;311(3):271–8.